Inside the DSO Revenue Gap
Vyne Dental’s Chief Product Officer Paul Bernard explores how leading DSOs identify, measure, and fix these gaps—and how you can too.
Many DSOs unknowingly lose thousands of dollars to inefficiencies hidden deep within their revenue workflows. From inaccurate coding to outdated collection processes, these “invisible leaks” can significantly impact the bottom line.
Whether you are running 50 offices or one, the RCM process is the same. However, the law of large numbers begins to affect DSOs as they grow.
“Every practice leaks, but these leaks really start showing up in a more magnified way the bigger you get,” Vyne Dental Chief Product Officer Paul Bernard says. “At the end of the day, if you see a patient and you expect to be paid $100, how much of that do you actually put in your pocket—and how much effort does it take to get those final pennies?”
Start with a Bigger Bucket
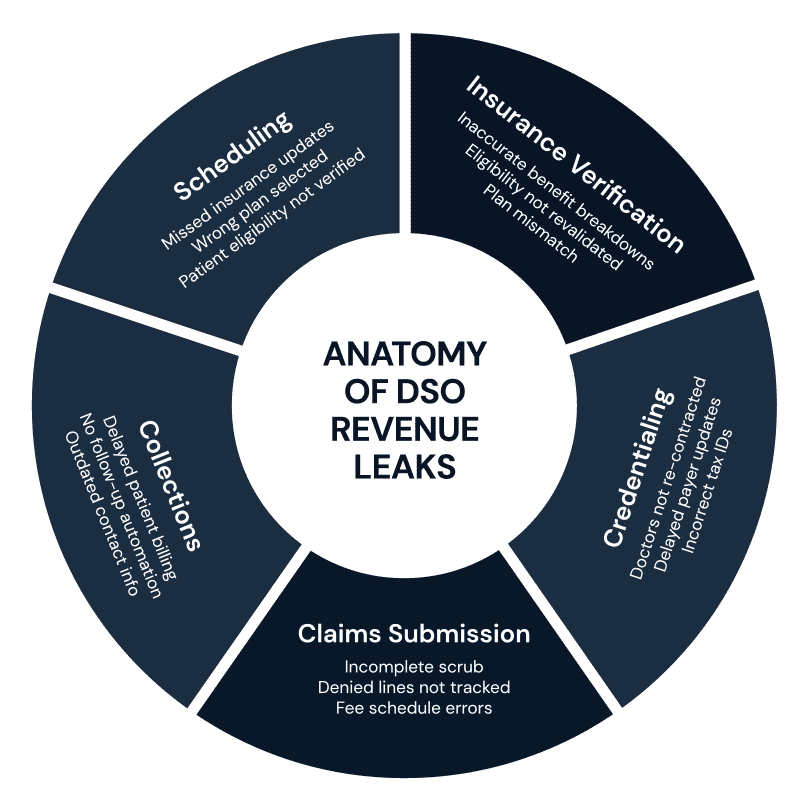
RCM starts long before billing a claim. The work you do up front to build a successful claim is part of the process. “People tend to want to bucket RCM too small. They think RCM is just billing the claims, which is just one piece. The whole process, from scheduling a patient to the patient making their final payment and everything in between, has aspects that significantly impact RCM,” Bernard explains.
By investing time on upfront processes in RCM, you can avoid spending energy on cleaning up mistakes. A process map can help you visualize that.
“Process mapping is not intuitive for a lot of people, but it’s no more complicated than examining what happens first, and then what happens next. You’ll start to see that prep work matters. It’s everything that happens before filing that makes that claim successful or not successful,” says Bernard.
Beyond mapping, narrowing your perspective on RCM can also limit your potential improvements.
“For instance, some think scheduling has no impact on RCM. It absolutely does,” Bernard notes. “I want to be looking for things at scheduling that will help me submit a successful claim, such as asking if patients have changed employers. Is their insurance still the same? If they don’t know, go ahead and schedule but loop back before they show up to see if you’re in network.
“If you have a narrow view of RCM,” Bernard points out, “you are going to find narrow opportunities to improve. All the things that must happen before you even send a claim to a payer contribute to how much you will be paid.”
Mistakes You Can’t Afford
Incomplete or Delayed Credentialing
One way DSOs can miss out on or delay revenue is failing to properly contract and credential doctors. This can significantly impact how and when they are paid.
When DSOs acquire a practice, payers have to be re-contracted, which usually happens under a different tax ID.
“Payers will send payments to a tax ID, not a doctor who’s in a location. Knowingly or unknowingly, you changed where the money gets routed, and your processes in RCM have to adjust for that,” Bernard explains. “Those claims won’t get paid because the insurance company doesn’t know who this doctor is. You’ve billed a claim that isn’t getting paid, and you end up having to unwind problems, which will cause delays in payment or denial of payment.”
Not Mining EOBs
Explanations of benefits (EOBs) are a tremendous source of process data because they will tell you what claim got denied, what line on a claim got denied, and why. If you understand those reasons, then you can see where in your process flow you could have caught it.
Inevitably, a lot of errors are going to be at the point where you validate whether the eligibility and benefits are accurate and before you make an estimation and choose a fee schedule. Find and fix that error—and get paid.
“It does you no good if you have a good eligibility and benefit breakdown but you’re picking the wrong plan for that patient. You are never going to get the exact amount correct, so maintaining these plans and payer plans and fee schedules in your practice management system is critical if you want to bring those two together,” Bernard explains.
Incomplete Claims
The ultimate goal is a clean claim with no receivables to manage. “You want to be collecting as much of what the patient owes up front as you can and then have some reasonable certainty that once you send that claim, it’s going to get paid whatever the insurance owes you,” notes Bernard.

“That’s a perfectly clean claim. That would mean that the level of effort that you must spend managing the receivable is zero because there is no receivable.”
Products like Vyne Trellis scrub claims before they get to the payer.
“It’s much better to try and put as much effort as you can up front to make sure that that claim is correct,” Bernard explains. “You can take 10 minutes now to fix it, or you can take two hours 30 or 60 days from now to try and figure out why you didn’t get paid. It’s a no-brainer—and yet somehow, we still allow these defects to escape the process.”
It’s All About Data
Don’t worry about making sure everyone is on the same practice management system.
“Why would you take a doctor who is unbelievably productive and generating revenue using whatever system they’ve been using and say, ‘Now that you’re part of a DSO, you need to switch.’?” Bernard asked. “Why would you rip out the wiring from somebody who is usually productive?”
The reality is that forcing a change often results in reduced productivity because staff are unfamiliar with the new system. It introduces unnecessary risk into the operation of a practice that was otherwise performing well.
Instead of focusing on uniformity of systems, DSOs should prioritize access to data. “Insist that the practice management systems give you your data,” he said. “Once you have it, you can bring that data into a centralized system and analyze it however you want. If you can free the data from those systems, you don’t need to change anything—and you reduce your operational risk.”
Once your data is accessible, you can measure performance across the organization without disrupting what Appointment Credentialing Claim Scrubbing Data Errors is already working. It’s not about the system itself—it’s about the visibility and control the data gives you.

Keep the Patient in the Loop
“You’ve got to think about the billing experience from the patient’s perspective,” says Bernard. “At Vyne Dental, we call it ‘patient in the loop.’”
If a patient leaves the doctor’s office, hears nothing for weeks, and then a surprise bill arrives, it can prompt confusion, doubt, and a timeconsuming call to the office. What if, instead, they were kept in the loop the whole time with clear, proactive updates? By the time the bill comes, they understand it, trust it, and are far more likely to pay it.
“There’s a direct correlation between time and payment,” Bernard explains. “The older that receivable gets, the less likely it is to be paid.”
When you build a billing process that moves efficiently, it not only benefits the patient but also strengthens the practice.
Build Smarter, Scale Stronger
RCM isn’t just billing—it’s a living ecosystem. And like any complex system, it’s only as strong as its weakest link. From initial patient scheduling to the moment a claim hits the payer, every step in the process either protects revenue or puts it at risk.
The most successful DSOs aren’t the ones who work harder to chase revenue—they’re the ones who build smarter systems to prevent loss before it happens. They invest in automation. They map out their processes. They scrub claims early. And they never stop analyzing their EOBs for trends that can unlock even greater efficiency.
Because at the end of the day, your revenue isn’t what you bill—it’s what you keep.
Strengthen your pipeline. Protect your bottom line. Scale with confidence. Experience Vyne Trellis®— the end-to-end revenue acceleration platform that gets you paid faster through streamlined claims submission and tracking, delivers batch and realtime eligibility checks, and keeps your communications secure.
Ready to Stop Revenue Leaks Before They Start?
Schedule your personalized demo today
at VyneDental.com.